Headaches and migraine are a common condition which can leave people feeling miserable and irritable, depressed and perhaps unable to manage day to day. The National Institute for Health and Clinical Excellence estimates that approximately 6 million people in the UK suffer from regular migraines, with around 190,000 migraine attacks happening every day. So what can we do to treat migraine?
How big a problem is migraine?

With around 190,000 migraine attacks taking place each day, migraine is clearly a widespread problem. Depending on the type and severity of your migraine the disruption to your everyday life can range from low-level discomfort to debilitating illness.
There are two main types of migraine – common and classic, some sufferers experience only one type, but many will experience both at one time or another.
Common Migraine
Which accounts for about 80-85% of attacks. Researchers think that a change in cerebral blood flow could be responsible for the symptoms of this headache, but there are still many questions about this theory.
Common migraine is more common in females, and normally involves:
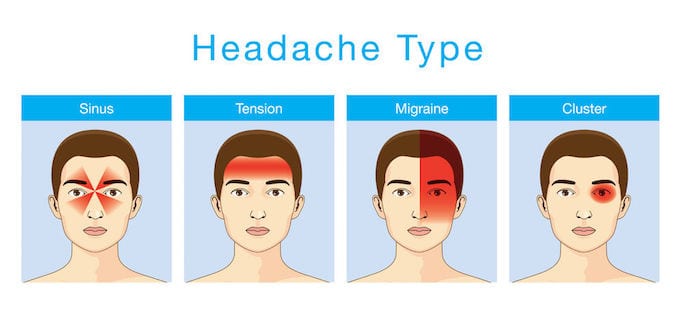
- a unilateral pulsing headache
- the onset of the condition in early adulthood
- low-level pulsing headache which continues perhaps for days
- periods of a severe headache which can be disabling
- associated nausea and vomiting.
Classic Migraine
The other type of migraine, classic migraine, accounts for about 10-15% of attacks. Classic migraine has essentially the same symptoms but is preceded by what is known as ‘aura’ or ‘prodrome’. This describes symptoms experienced prior to the onset of the throbbing headache such as:
- visual symptoms such as flashing lights (scintillation)
- the presence of a blind spot (scotoma).
This usually lasts up to 30 minutes after which it is replaced by the familiar symptoms of common migraine, which can last for a few hours to 3 days.
Photophobia (sensitivity to bright lights) is common and bright lights can also provoke the pain. Again, the cause of these headaches are not fully understood but are thought to be related to the changes in blood flow, the presence of certain chemicals and the way in which nerves send signals.
Many migraine sufferers report specific triggers which tend to set their migraine off – these include:
- Periods of stress, and after periods of stress (commonly occurs on over the weekend or holidays)
- Some foods (commonly; chocolate, caffeine, nitrates, cheese, nuts and wine)
- Some medications
- Changes in sleeping habits
- Hormonal changes (associations with the menstrual cycle)
- Tension in the neck and neck pain (especially the upper part of the neck)
Do medications cure headaches?
While many people turn to medication to treat migraine, is this really an effective way to go?
Paracetamol is a common an easily available choice for treating all kinds of pain – especially spinal pain. The theory is often that reducing neck pain might help to stop migraine. In fact, research suggests it isn’t particularly effective at doing this. A recent systematic review including three randomised controlled trials focused on spinal pain, concluded that there was high-quality evidence that paracetamol was no more effective than placebo in this instance[1]
A further typical approach is to reach for Non-steroidal anti-inflammatory drugs or NSAIDs. Unlike paracetamol, evidence shows that NSAIDs can have a positive effect for some conditions – A systematic review including 35 randomised trials found moderate- quality to high-quality evidence that NSAIDs reduce spinal pain by about 6 points, and chronic non-specific low back pain specifically by about 11 points, on a 100-point scale.[2]
If your migraines are being triggered by neck pain, NSAID’s, therefore, might help – The problem is that 11 points or reduction, while something, is not very much. Indeed, the same study concluded that overall the effects are too small to be considered worthwhile by the typical patient. NSAID usage must also be balanced against the risk of long-term consumption – some studies have shown evidence that NSAIDs may slightly increase the risk of heart problems, and it is well known that they carry well-known gastrointestinal and renal risks.
Another, stronger option are opioids, which are commonly prescribed for pain management in all kinds of conditions from migraine to back pain. While opioid medications are effective in reducing pain, they come with serious side effects. Because of this their are still a lack of studies investigating just how effective they might be for migraine sufferers. One of the biggest obstacles to performing such studies has been the fact that more than half of patients cannot even tolerate opioids and remain well enough to stay in a trial – let alone rely on them as a long-term solution.[3]
What’s more, the potential for developing serotonin syndrome (which can be life-threatening, and consists of a combination of mental status changes, neuromuscular hyperactivity, and autonomic
hyperactivity) is relatively high in the patients who are using opioids for pain control. Because of these risks, the use of opioids in migraine headache is already discouraged, especially when we take into account the associated risk of medication overuse headache and also an increase in headache-related disability[4][5]
A better solution for headache and migraine
If medication isn’t the best approach to treating migraine, what is? One of the most promising options is Chiropractic care. Spinal manipulation, a process of gently guiding the spinal bones back into the correct alignment, is the primary treatment method of most chiropractors – but more advanced clinics like Complete Chiropractic can also utilise methods such as chiropractic biophysics to be even more effective.
Unlike the drug based approaches, chiropractic care has no side effects, and there is a growing body of evidence which suggests that chiropractic care can have real benefit for migraine sufferers.
For example, a study reported on in the Journal of Manipulative and Physiological Therapeutics in February of 2000, which considered 127 participants showed that after two months of chiropractic treatment, 22 per cent of the participants reported more than a 90 per cent reduction of their migraines. Approximately 50% more participants reported significant improvement in the duration and severity of each episode – which means that overall, 70% of people experience a significant improvement in their symptoms after only a few sessions of chiropractic care.
If you’re suffering with migraine, why not follow the evidence and give chiropractic a try? Take advantage of our new patient special or speak to your chiropractor today!
[1] Machado GC, Maher CG, Ferreira PH, et al. Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis
[2] Abdel Shaheed C, Maher CG, Williams KA, et al. Efficacy, tolerability, and dose-dependent effects of opioid analgesics for low back pain: a systematic review and meta-analysis. JAMA Intern Med 2016;176:958–68.
[3] Abdel Shaheed C, Maher CG, Williams KA, et al. Efficacy, tolerability, and dose-dependent effects of opioid analgesics for low back pain: a systematic review and meta-analysis. JAMA Intern Med 2016;176:958–68.
[4] Hossein Ansari, Leila Kouti, Drug Interaction and Serotonin Toxicity with Opioid Use: Another Reason to Avoid Opioids in Headache and Migraine Treatment Curr Pain Headache Rep (2016) 20: 50.
[5] Katsarava et al. Neurology 62:788-790, 2004; Bigal and Lipton. Neurology 71:1821-8, 2008; Casucci and Cevoli. Neurol Sci. 34 Suppl 1:S125-8, 2013
